






L. Kamel,1 A. Morsy1 and A. El Shamaa2
إنتاج سيتوكين الخلايا التائية وخلل وظيفة البطانة لدى السكريـين من النمط 2 المصابين باعتلال الكلية
ليلى كامل، عبد الله مرسي، عزة الشماع
الخلاصـة: قيَّم الباحثون في هذه الدراسة التغيرات في مستويات السيتوكينات للأنتـرفيرون γ والانتـرلوكين - 10 (وهي واسمات بيولوجية للتغير الالتهابي) مع الواسمات البيولوجية الذوَّابة sICAM-1 وسيليكتن sE (وهي واسمات بيولوجية لخلل وظيفة البطانة) لدى السكريـين سواء مصابين أو غير مصابين باعتلال الكلية. ولاحظ الباحثون ازدياداً ملحوظاً في كل من الانتـرفيرون γ والانتـرولوكين - 10 لدى السكريـين المصابين باعتلال الكلية وأولئك الذين لديهم مرضاً كلوياً في مرحلته النهائية، وذلك بالمقارنة مع الشواهد ومع المرضى غير المصابين باعتلال الكلية. وقد حصل ازدياد يُعْتَدُّ به في كل من الانتـرفيرون γ والانتـرلوكين - 10 بعد الديال الدموي. أما sICAM-1 وسيليكتن sE فقد كانت أعلى بمقدار يُعْتَدُّ به لدى السكريـين ومجموعات المصابين باعتلال الكلية السكري والمرض الكلوي في مرحلته النهائية بالمقارنة مع الشواهد، وكان sICAM-1 أعلى بعد الديال الدموي ولم يكن سيليكتن sE أعلى بعد الديال الدموي.
ABSTRACT This study assessed changes in serum levels of cytokines IFNγ and IL-10 (biomarkers of inflammatory changes) and soluble biomarkers sICAM-1 and sE-selectin (biomarkers of endothelial dysfunction) in diabetic patients with and without nephropathy. IFNγ and IL-10 were significantly elevated in patients with diabetic nephropathy (DN) and end-stage renal disease (ESRD) compared with controls and diabetic patients without DN. IFNγ and IL-10 levels were significantly increased after haemodialysis. sICAM-1 and sE-selectin were significantly higher in diabetic, DN and ESRD groups compared with controls, and sICAM-1 but not sE-selectin was increased after haemodialysis.
La production de cytokines par les cellules T et du dysfonctionnement endothélial chez les sujets diabétiques de type 2 atteints de néphropathie
RÉSUMÉ Cette étude a permis d'évaluer les modifications des taux sériques de cytokines IFNγ et IL-10 (biomarqueurs de modifications de l’état inflammatoire) et de biomarqueurs solubles sICAM-1 et sE-sélectine (biomarqueurs du dysfonctionnement endothélial) chez des patients diabétiques atteints et non atteints de néphropathie. Les IFNγ et les IL-10 étaient significativement élevés chez ceux qui présentaient une néphropathie diabétique (ND) et une maladie rénale en phase terminale (MRPT) par rapport aux témoins et aux patients diabétiques sans ND. Les niveaux d’IFNγ et d’IL-10 avaient augmenté de façon significative après l’hémodialyse. Le taux de sICAM-1 et de sE-sélectine étaient significativement plus élevés dans les groupes atteints de diabète, de ND et de MRPT par rapport aux témoins, et ceux de sICAM-1 mais pas de sE-sélectine avaient augmenté après l’hémodialyse.
1Department of Clinical Chemistry; 2Department of Nephrology, Theodor Bilharz Research Institute, Cairo, Egypt (Correspondence to L. Kamel:
Received: 02/12/06; accepted: 28/03/07
EMHJ, 2009, 15(4): 807-816
Introduction
Diabetic nephropathy (DN) is a leading cause of chronic renal failure and is a growing concern given the increasing incidence of type 2 diabetes. For diabetic patients on haemodialysis (HD), dysfunction of the host defences against infection has major clinical and socioeconomic implications.
The autoimmune nature of diabetes and the major contribution of lymphocyte T-cells are well established. However, the mechanism of this immune dysregulation is still unclear. T-cells have 2 subsets of helper cells: T-helper type 1 (Th1) and type 2 (Th2). Th1 cells are effectors of cell-mediated immunity, secreting the cytokine interferon-gamma (IFNγ) that inhibits Th2 cell differentiation. Th2 cells produce cytokine interleukins IL-4 and IL-10, which inhibit IFNγ secretion and cell immunity [1]. An altered balance of Th1/Th2 may be associated with the pathogenesis of end-stage renal disease (ESRD) [2] and with impaired immunity in HD patients [3]. Both IFNγ and IL-10 play major roles in the regulation of immune and inflammatory responses; in a model of chronic renal disease IL-10 blocked inflammation and improved renal function [4].
Vascular damage is frequently observed in patients with chronic renal failure and under HD, and disturbances in endothelial function may play a role in vascular complications such as stroke or ischaemic heart disease. Malyszko et al. found evidence of endothelial cell injury in renal failure patients, particularly those on continuous ambulatory peritoneal dialysis, and a high degree of hypercoagulation relative to healthy subjects [5]. This may lead to fibrin deposition in the vascular wall, thrombus formation, and the development and progression of atherosclerosis with its complications. Several markers of endothelial cell activation—including soluble intercellular adhesion molecule (sICAM-1), von Willebrand factor, soluble E-selectin (sE-selectin), and soluble thrombomodulin—are providing further evidence of the relationship between endothelial cell activation and damage to the vasculature in diabetes [6].
The purpose of the present study was to assess the changes in serum levels of the pro-inflammatory cytokine IFNγ and anti-inflammatory cytokine IL-10 (as markers of inflammatory changes) and the soluble biomarkers sICAM-1 and sE-selectin (as markers of endothelial dysfunction) in diabetic patients with and without nephropathy. We also evaluated the effect of renal dialysis on these mediators. Such information is crucial to determine the optimal approach to improve the immune response of DN patients which might reduce the morbidity and mortality due to infection.
Methods
Patients
The study was carried out on 73 subjects selected from the Nephrology Department and Dialysis Unit of Theodor Bilharz Research Institute, Cairo. Subjects were categorized into groups as follows:
- Diabetic group (n = 17): patients with type 2 diabetes without renal involvement (normoalbuminuria). The diagnosis of type 2 diabetes was established before they were screened for the study and they did not require insulin therapy for glucose control. Diabetes was defined according to the recommendations of the American Diabetes Association Expert Committee on the Classification and Diagnosis of Diabetes [7].
- Diabetic nephropathy (DN) group (n = 22): patients with type 2 diabetes with renal involvement. The inclusion criteria were: lower limb oedema, proteinuria, impaired renal function and normal-sized kidney with increased echogenicity on abdominal ultrasound.
- ESRD group (n = 19): patients with type 2 diabetes with ESRD before the start of dialysis sessions. Data for these patients were collected before and after 10 sessions of HD. Dialysis (4 hours duration) was done 3 times/week with haemophan membranes using acetate solution.
- Control group (n = 15): volunteers recruited from those attending outpatient clinics for check-ups and who had no medical disorders in a health examination.
Data collection
All subjects underwent the following: full history-taking, thorough clinical examination, abdominal ultrasonography, fundus examination and electrocardiography. Venous blood samples were withdrawn from the anticubital vein from all subjects in the morning after 12 hours overnight fasting. Routine tests were performed immediately and aliquots were stored at –60 °C for further estimation of serum levels of IFNγ, IL-10, sICAM-1 and sE-selectin.
The routine laboratory investigations performed by conventional methods included:
- Complete blood count, fasting and postprandial blood glucose and routine urine analysis for all groups and microalbumin for those with negative protein in the urine. Normoalbuminuria was defined as spot urine albumin/creatinine ratio < 30 µg/mg, whereas macroalbuminuria was defined as spot urine albumin/creatinine ratio > 300 µg/mg. This ratio is regarded as one of the best indicators of urinary albumin excretion and is recommended by the American Diabetes Association [7].
- Liver function tests: serum aminotransferase, alkaline phosphatase, albumin, bilirubin and prothrombin concentration.
- Kidney function tests: serum creatinine, urea, sodium, potassium, calcium and phosphorus.
- Lipid profile: total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and triglycerides.
- The following special laboratory tests were carried out:
- Serum IFNγ was performed by a solid-phase sandwich enzyme linked-immunosorbent assay (ELISA) (Diaclone Research, France). The lower detection limit of the assay is < 5 pg/mL and there is no cross-reactivity with other human cytokines.
- Serum IL-10 was assayed by a solid-phase sandwich ELISA (Diaclone Research, France). The lower detection limit of the assay is < 5 pg/mL and it recognizes both natural and recombinant human IL-10.
- Serum sICAM-1 was assayed using a solid-phase sandwich ELISA (Diaclone Research, France). The lower detection limit of the assay is < 0.1 ng/mL and there is no cross-reactivity with other human adhesion molecules
- Soluble sE-selectin was performed with a quantitative sandwich ELISA (R&D Systems, MN, United States of America). The minimum detectable dose of sE-selectin is typically < 0.1 ng/mL and no significant cross-reactivity is observed with natural human IgG or natural human P-selectin.
Statistical analysis
Numerical data were expressed as mean and standard deviation (SD). Multiple intergroup comparisons were made using 1-way ANOVA. If a significant change was found in intergroup comparisons, post hoc multiple comparison analysis with the Tukey–Kramer multiple comparison test was performed. Correlations were computed using the Spearman correlation coefficient. P values < 0.05 were considered statistically significant. SPSS, version 10 for Windows, was used for data analysis.
Results
Table 1 shows the clinical characteristics and laboratory data of the four study groups. Serum creatinine showed a statistically significant elevation in the ESRD group compared with the control, diabetic and DN groups (P < 0.001). Fasting blood glucose levels were significantly higher in diabetic, DN, and ESRD groups compared with the control group (P < 0.001, P < 0.001, P < 0.05 respectively).
IFNγ showed a significant elevation in both the DN and ESRD groups compared with the control group (P < 0.01) and diabetic group (P < 0.05) (Figure 1). IL-10 also showed a significant elevation in both DN and ESRD groups versus the control and diabetic groups (P < 0.001) (Figure 1). Both IFNγ and IL-10 levels were significantly increased after initiation of HD when compared with their values in the ESRD group before the start of dialysis (P < 0.05 and P < 0.01 respectively).
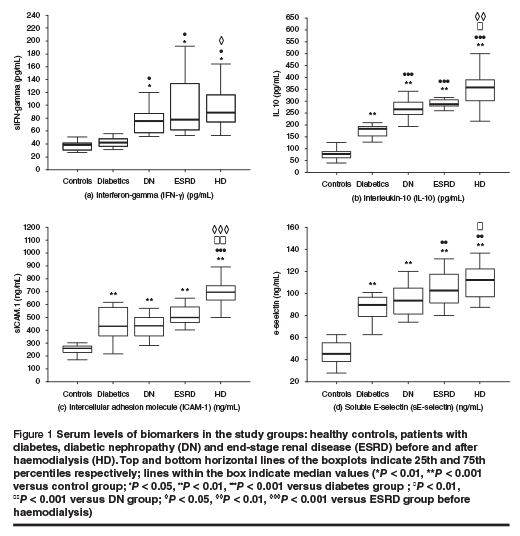
We found a significant elevation in sICAM-1 and sE-selectin in diabetic, DN and ESRD groups compared with the control group (P < 0.001). Soluble ICAM-1, but not sE-selectin, showed a statistically significant increase after HD initiation when compared with its level in ESRD before the start of dialysis (P < 0.001) (Figure 1).
There was a positive correlation between the levels of IFNγ and IL-10 (r = 0.444, P < 0.01) (Figure 2). Our study showed a positive correlation between sICAM-1 and serum creatinine (r = 0.362, P < 0.05). We also found a positive correlation between E-selectin and both serum urea (r = 0.330, P < 0.05) and serum creatinine (r = 0.309, P < 0.05)
 and serum interferon-gamma (IFNgamma) levels in all 41 patients with diabetic nephropathy (n = 22) and end-stage renal disease (n = 19) (r = 0.444, P < 0.01)")
Discussion
DN is a leading cause of ESRD and is a growing concern given the increasing incidence of type 2 diabetes. The suggested causes of inflammation in ESRD include decreased renal function, volume overload, co-morbidity, factors associated with the dialysis procedure and genetic factors [8]. An altered balance of Th1/Th2 and endothelial dysfunction has been associated with ESRD [9].
In our study, IFNγ (reflecting Th1 activity) and IL-10 (reflecting Th2 activity) showed significant elevations in both DN and ESRD groups compared with both the control group and patients with diabetes. This agrees with another study on the effects of renal failure on the Th1/Th2 lymphocyte profile which showed that the intracellular content of IFNγ, IL-2, IL-4, and IL-10 was significantly higher in patients with chronic renal failure [10]. Our results also agree with studies on renal failure patients in whom spontaneous activation of T-lymphocytes was detected [11,12].
Our study revealed that both IFNγ level and IL-10 levels were significantly increased after initiation of HD when compared with their values in the ESRD group before the start of dialysis. Daichou et al. also found that IFNγ production by Th1 cells was significantly higher in HD patients yet, in contrast, they showed that production of IL-4 and IL-10, which affect humoral immunity, were significantly lower in HD patients than in controls. They concluded that cellular immunity induced by Th1 and humoral immunity induced by Th2 are both decreased in HD patients, but that improved IL-12 secretion by macrophages activates natural killer cells to produce IFNγ, which in turn induces macrophage activity [11].
In contrast to our results, Pupim et al. found that initiation of maintenance HD did not significantly influence plasma concentrations of IL-10, suggesting that HD is ineffective in controlling inflammation and oxidative stress in renal failure [13]. However, Brunet et al. demonstrated increased spontaneous synthesis and secretion of IL-10 in HD patients, which is evidence of the well-documented state of activation of monocytes and lymphocytes in HD patients due to contact with the dialyser membrane [14].
Girndt et al. explained the increased IL-10 levels in HD patients in their study as due to the fact that in healthy subjects there is a distinct population of monocytes producing exclusively IL-10 when stimulated, but that these regulating monocytes are reduced in dialysis patients so that there is overproduction of pro-inflammatory factors [15]. Fodor et al. demonstrated higher levels of IFNγ in CD4+ T-cells of HD patients, explained by activation of peripheral T-cells with increased production of Th1 cytokines (IFNγ, IL-2) and decreased synthesis of Th2 cytokines (IL-4, IL-13) [16]. They explained the elevated expression of IL-10 in CD4+ and CD8+ (Th2) cells as a counter-regulatory Th2 activation in response to the Th1 effect.
The results of our study show that both the pro-inflammatory cytokine IFNγ and the potent anti-inflammatory cytokine IL-10 were significantly elevated in DN and ESRD patients as compared to diabetic patients. We explain this concomitant rise of both cytokines by the fact that increased production of IL-10 may represent an autoregulatory response to increased production of pro-inflammatory cytokines by monocytes. We also found a more pronounced increase of both cytokines after HD sessions as evidence of the activation of monocytes and lymphocytes due to contact with the dialyser membrane.
In our study the levels of the soluble endothelial markers serum sICAM-1 and sE-selectin showed a significant increase in the diabetic, DN and ESRD patient groups as compared with the control group, which is in accordance with previous data demonstrating that serum levels of sICAM-1 and sE-selectin were elevated in diabetic patients [17,18] and undialysed patients with chronic renal failure [5,19–21]. Our results contrast, however, with other workers who found a non-significant rise in serum sE-selectin levels in ESRD patients [22], and no elevation of sICAM-1 levels in type 2 diabetic patients [23,24]. The discrepancy among studies regarding the levels of soluble serum endothelial markers in diabetes could be attributed to differences in the number of patients studied, their physical characteristics, the grade of metabolic control, the presence of hypertension or lipid levels.
Levels of the soluble adhesion molecule ICAM-1 showed a statistically significant increase after the start of HD compared with its level in ESRD patients before the start of dialysis. Similarly, elevated sICAM-1 levels in HD patients were previously demonstrated [19,25–27]. Others found that sICAM-1 levels post-HD were significantly higher than pre-HD and suggested that sICAM-1 is shed from the surface of mononuclear cells (lymphocytes and monocytes) and released into the circulation stimulated by dialysis membranes [28]. The significant increase in ICAM-1 levels in HD patients indicates that its membrane-adsorptive properties do not exert a major influence on its clearance. In view of the large size of the molecule it is unlikely that it could be cleared intact through the membranes used.
On the other hand, no significant elevation in E-selectin levels was detected after initiation of HD compared with ESRD values before the start of HD. This result contrasts with previously published data from patients on continuous ambulatory peritoneal dialysis or HD [21].
Our study showed a positive correlation between sICAM-1 and serum creatinine in DN and ESRD patients (r = 0.362). This is in accordance with other researchers, who found that in undialysed patients with chronic renal failure the levels of serum sICAM-1 increased with decreasing renal function [19,25]. We also found a positive correlation between E-selectin and both serum urea (r = 0.330), and serum creatinine in DN and ESRD patients (r = 0.309). Similarly, others have found a linear relation between serum creatinine and adhesion molecule levels [29]. These findings suggest that the kidney may play an important role in the catabolism of adhesion molecules.
Our results concerning markers of endothelial cell activation could be explained by the effects of cytokines on the endothelium or by reduced clearance of endothelial products. However, since renal dysfunction was the primary abnormality, it is likely that increases in sICAM-1 and sE-selectin are secondary to CRF. This is supported by the correlation between soluble endothelial cell markers and creatinine levels, suggesting that renal clearance may affect circulating cytokine levels. In dialysed patients, there was no reduction in the levels of sE-selectin, which are large enough to be excluded from dialysis, and the levels of sICAM-1 were further increased.
We also found a positive correlation between the levels of IFNγ and IL-10 in DN and ESRD patients (r = 0.44). IL-10 is known as the most important anti-inflammatory cytokine found in the human immune response and its activity acts as an inhibitory factor in cytokine synthesis; yet several studies have suggested IL-10 has immunostimulatory properties [30]. Our results are in accordance with a study that reported a direct correlation between serum IL-10 values and those of IFNγ in HD patients, suggesting an immunomodulatory role of IL-10 in this setting [31]. We conclude that the production of IL-10 represents an autoregulatory response to the increased production of the pro-inflammatory cytokines by monocytes.
In conclusion, although other pro- and anti-inflammatory cytokines may be of importance, our data suggest that the anti-inflammatory cytokine IL-10 and the proinflammatory cytokines IFNγ play important roles in the development of T-helper cell imbalance in renal failure. The reasons for the increased risk of inflammation in diabetic ESRD patients appear to be complex, including non-dialysis- as well as dialysis-related factors. The combination of an impaired immune response and persistent immune stimulation are factors in the low-grade systemic inflammation and altered cytokine balance that characterize renal failure and which may result in an increased risk of vascular disease. Several interrelated processes are involved in DN, such as oxidative stress, endothelial dysfunction and vascular calcification, in an environment of constant low-grade inflammation, with an altered balance of Th1/Th2 cells as well as a dysregulated cytokine network. Further studies are needed to evaluate whether general or targeted anticytokine treatment strategies could be effective in diabetic patients with ESRD. Also therapies that improve endothelial dysfunction may prove important in management of type 2 diabetes and its costly, morbid complications.
References
- Libetta C, Rampino T, Canton AD. Polarization of T-helper lymphocytes toward the Th2 phenotype in uremic patients. American journal of kidney diseases, 2001, 38(2):286–95.
- Nitta K et al. Characterization of TH1/TH2 profile in uremic patients. Nephron, 2002, 91(3):492–5.
- Daichou Y et al. Characteristic cytokine products of Th1 and Th2 cells in hemodialysis patients. Nephron, 1999, 83(3):237–45.
- Mu W et al. IL-10 suppresses chemokines, inflammation, and fibrosis in a model of chronic renal disease. Journal of the American Society of Nephrology, 2005, 16(12):3651–60.
- Malyszko J, Malyszko J, Mysliwiec M. Endothelial cell injury markers in chronic renal failure on conservative treatment and continuous ambulatory peritoneal dialysis. Kidney and blood press research, 2004, 27(2):71–7.
- Blann A, Lip G. Endothelial integrity, soluble adhesion molecules and platelet markers in type 1 diabetes mellitus. Diabetic medicine, 1998, 15(8):634–42.
- American Diabetes Association. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes care, 1997, 20:1183–97.
- Stenvinkel P. Inflammation in end-stage renal disease––a fire that burns within. Contributions to nephrology, 2005, 149:185–99.
- Stenvinkel P et al. IL-10, IL-6, and TNF-alpha: central factors in the altered cytokine network of uremia—the good, the bad, and the ugly. Kidney international, 2005, 67(4):1216–33.
- Alvarez-Lara M et al. The imbalance in the ratio of Th1 and Th2 helper lymphocytes in uraemia is mediated by an increased apoptosis of Th1 subset. Nephrology, dialysis, transplantation, 2004, 19:3084–90.
- Daichou Y et al. Characteristic cytokine products of Th1 and Th2 cells in hemodialysis patients. Nephron, 1999, 83:237–45.
- Sester U, Sester M, Hauk M. T-cell activation follows Th1 rather than Th2 pattern in haemodialysis patients. Nephrology, dialysis, transplantation, 2000, 15:1217–23.
- Pupim L et al. Influence of initiation of maintenance hemodialysis on biomarkers of inflammation and oxidative stress. Kidney international, 2004, 65:2371–9.
- Brunet P et al. IL-10 synthesis and secretion by peripheral blood mononuclear cells in haemodialysis patients. Nephrology dialysis transplantation, 1998, 13:1745–51.
- Girndt M et al. Production of proinflammatory and regulatory monokines in hemodialysis patients shown at a single-cell level. Journal of the American Society of Nephrology, 1998, 9:1689–96.
- Fodor B et al. No effect of transfusion transmitted virus viremia on the distribution and activation of peripheral lymphocytes in hemodialyzed patients. Nephron, 2002, 92:933–7.
- Glowinska B et al. Soluble adhesion molecules (sICAM-1, sVCAM-1) and selectins (sE selectin, sP selectin, sL selectin) levels in children and adolescents with obesity, hypertension, and diabetes. Metabolism, clinical and experimental, 2005, 54(8):1020–6.
- Leinonen E et al. Low grade inflammation, endothelial activation and carotid intima media thickness in type 2 diabetes. Journal of internal medicine, 2004, 256:119–27.
- Bonomini M et al. Serum levels of soluble adhesion molecules in chronic renal failure and dialysis patients. Nephron, 1998, 79:399–407.
- Güler S et al. Plasma soluble Intercellular adhesion molecule 1 levels are increased in type 2 diabetic patients with nephropathy. Hormone research, 2002, 58:67–70.
- Musia K et al. Serum VCAM-1, ICAM-1, and L-selectin levels in children and young adults with chronic renal failure. Pediatric nephrology, 2005, 20:52–5.
- Bolton CH et al. Endothelial dysfunction in chronic renal failure: roles of lipoprotein oxidation and pro-inflammatory cytokines. Nephrology dialysis transplantation, 2001, 16:1189–97.
- Viswanathan V et al. Markers of endothelial dysfunction in hyperglycaemic Asian Indian subjects. Journal of diabetes and its complications, 2004, 18:47–52.
- Boulbou M et al. Circulating adhesion molecule levels in type 2 diabetes mellitus and hypertension. International journal of cardiology, 2005, 98:39–44.
- Papayianni A et al. Circulating levels of ICAM-1, VCAM-1, and MCP-1 are increased in haemodialysis patients: association with inflammation, dyslipidaemia, and vascular events. Nephrology, dialysis, transplantation, 2002, 17:435–41.
- Rabb H et al. Alterations in soluble intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 in hemodialysis patients. American journal of kidney diseases, 1996, 27:239–43.
- Thylen P et al. Monocyte and granulocyte CD11b/CD18, CD62L expression and sICAM-1 concentration in the interdialytic period. Nephron, 1996, 74:275–82.
- Kawabata K et al. Changes in soluble ICAM-1 level during hemodialysis. Nippon jinzo gakkai shi, 1995, 37:632–8.
- Pecoits-Filho R et al. Associations between circulating inflammatory markers and residual renal function in CRF patients. American journal of kidney diseases, 2003, 41:1212–8.
- Lelievre D et al. Preincubation of human resting t cell clones with interleukin 10 strongly enhances their ability to produce cytokines after stimulation. Cytokine, 1998, 10:831–40.
- Allam MN, Radwan AS, Waked E. Hemophan hemodialysis promotes the inflammatory state of uremia. Kasr El Eini medical journal, 2005, 11(6):220.