






Sélectionnez votre langue
Support to health facilities
5 years of war in Yemen has left its health system on the brink of collapse. Only 50% of health facilities are fully functioning.

WHO, in coordination with health authorities and partners, scaled up the response in 2019 by increasing the provision of medicines, fuel and life-saving supplies.
This support helps to keep the health system functional and provide access to health care.
This critical support of fuel to health facilities was made possible through the generous fund of the World Bank through the Emergency Health and Nutrition Project, the King Salman Humanitarian Aid and Relief Centre, United Arab Emirates Aid, Yemen Humanitarian Fund and the Office of U.S. Foreign Disaster Assistance.

Fuel distribution to health facilities in Yemen by WHO in 2019
Nutrition
Based on the Humanitarian Response Plan Yemen 2025, about 8.6 million children under-five and pregnant and lactating women (PLWs) are in need of humanitarian nutrition support. An estimated 2.3 million children are wasted and are in need of timely, quality treatment for acute malnutrition, alongside 1.3 million malnourished pregnant and breastfeeding women. Similarly, 2.1 million children under five are stunted and at risk of losing their future due diminished educational performance and reduced productivity in adulthood. 500,000 children under five are in need of quality lifesaving treatment for severe wasting including 53,000 children with severe acute malnutrition with medical complications.

Support in TFCs is not limited to life-saving services. It also extends to preventive measures, through the provision of extensive infant and young child feeding counselling for caregivers, which seeks to:
protect and promote breastfeeding and appropriate complementary feeding.
prevent relapses, and similar episodes in other children within the family; and
promote health and nutrition care-seeking behaviour among caregivers for the healthy growth of children aged under 5 years.
WHO ensures the provision of medical and non-medical supplies to all TFCs and covers their running costs. It also covers the referral cost for caregivers, to avoid or reduce their out-of-pocket expenses and improve caregiver compliance with treatment.
From January to June, performance indicators in WHO-supported TFCs in Yemen were as below:
Number of children admitted to WHO supported 96 TFCs: 12,478
Proportion of children admitted aged under 6 months: 18% (2,252 children)
Proportion of admitted children stabilized and referred to an outpatient therapeutic programme: 97% (11,415 children)
Death rate: 1% (81 children)
Number of caregivers benefiting from infant and young child feeding counselling sessions in TFCs: 12,478
Relapse Rate: 3% (313 children)
TFCs link with referral paediatric wards for the most serious cases of Moderate acute malnutrition (MAM) with comorbidities. In 2025, January to June, 2,754 children with acute and moderate malnutrition were admitted to a paediatric ward.
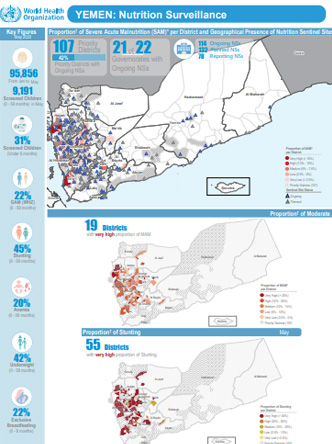
Nutrition surveillance

Under the nutrition surveillance system, nutritional assessment is usually performed through consideration of the child’s age and the measurement of the child’s weight, height/length, mid-upper arm circumference, haemoglobin level, breastfeeding status, and oedema.
It is a facility-based surveillance system, established mainly in district hospitals across the country and through trained health workers. The system provides the proportion of children aged under 5 years with any form of malnutrition out of the total children screened. The results only reflect the status of children who have attended a health facility or screening site during the month under review. The system tracks 4 out of 6 global core nutrition indicators: wasting, stunting, exclusive breastfeeding and anaemia.
A monthly bulletin is shared with all stakeholders at the national, regional and global levels for information and to support decision-making.
59,273 children aged under 5 years were screened (23% aged under 6 months);
27% of children were wasted and referred to an appropriate nutrition programme: Hodeidah had the highest proportion of acute malnutrition among children screened (46%);
47% of children were underweight;
chronic malnutrition (stunting) remains of high concern, affecting 41% of screened children and reflected in high proportions of stunting among children in 161 districts;
anaemia was confirmed in 23% of children aged 6–59 months screened for anaemia; and
exclusive breastfeeding among infants aged under 6 months showed a very low average rate (14%), which lags far behind the WHO global target for 2025 (at least 50%) and suggests causal linkages between suboptimal breastfeeding practices and high levels of acute and chronic malnutrition.
Polio
Polio is a highly contagious viral disease that mainly affects children and can cause permanent, lifelong paralysis. Over three decades, the Global Polio Eradication Initiative has worked with governments and partners to slash the number of polio cases from hundreds of thousands worldwide, to several dozen. But polio anywhere is a threat to children everywhere, and in places where immunity levels are lower than they should be, the risk of a polio outbreak is high. The way forward is to vaccinate all children with oral polio vaccine (OPV) so that the virus has nowhere to go and dies out.

Yemen has long maintained a vigilant polio surveillance system, consistently meeting or exceeding the two international indicators of effectiveness.
Even when a country is not in an outbreak situation, regular vaccination campaigns are conducted to maintain high immunity levels – Yemen’s last was in December 2019.
Yemen’s current outbreak is caused by the vaccine-derived poliovirus type 1 strain, which emerges in communities where not enough children have been vaccinated.
Outbreak response includes three rounds of vaccination, targeting all children under age 5.
In the first round of response, vaccinators gave polio drops to more than 5.1 million children.
Eleven percent of children vaccinated were aged under one year and received polio drops for the first time.
Plans are under way to improve Yemen’s laboratory testing capacity, one of the foundations of a robust polio surveillance system.
Nutrition
The ongoing conflict and resulting economic crisis are the main drivers of food insecurity in Yemen leaving the country’s critical civil infrastructure in ruins.

To save lives, WHO, in collaboration with local health authorities and, through the Emergency Health and Nutrition Project funded by the World Bank have established a nutrition surveillance system to find and refer for the appropriate treatment all children affected by acute malnutrition. The nutrition surveillance system prioritizes and closely monitor communities at elevated risk of famine. The system is designed to find the lives we so desperately need to save.
Nutritional assessment in the nutrition surveillance system is normally performed through the measurement of child’s weigh, height/length, measurement of upper arm circumference, age, haemoglobin level, breastfeeding status and oedema. It is a Facility-based surveillance system, established mainly in district hospitals across the country. The system provides the proportions of children under five years found suffering from any forms of malnutrition, out of the total children screened. The results only reflect the status of children who have attended the health facility in the month under review. The system tracks 4 out of 6 global core nutrition indicators: stunting, wasting, exclusive breastfeeding, and anaemia.
In 2020 because of COVID-19 to mitigate the risk of hospital-acquired infection, adapted protocol have been put in place to ensure safe screening services and minimize cross infections while performing a correct assessment. Therefore, some indicators, e.g. acute malnutrition by weight-for-height Z-score and stunting, were temporarily excluded from the set of measurements, as an interim measure to control the spread of infection, although the use of anthropometric tools is safe after sanitization. Currently, although some sites are still following these operating procedures, most of the sentinel sites have resumed the assessment of all indicators.
Each month a bulletin is produced and widely shared with all stakeholders at national, regional, and global level for information sharing and to support decision-making.
Key actions in 2021
From January to February 2021, 134 247 children under 5 years were screened for malnutrition across the 249 nutrition surveillance sites established in Yemen.
For the month of February, 63 345 were screened with 23% were under 6 months of age. 22% were found suffering from wasting and referred to the appropriate nutrition programmes, Hodidah had the highest proportions of acute malnutrition, and 47% were underweight.
Chronic malnutrition (stunting) remains of high concern affecting 44% of screened children and reflected in high proportions in 149 districts. 19% of 6-59 month children have anemia, and exclusive breastfeeding among infants under 6 months of age shows very low average rates 15% which still lags behind the WHO global targets 2025 (at least 50%) suggesting causal linkages between sub-optimal breastfeeding practices and high levels of acute and chronic malnutrition.
Expanded Programme on Immunization

Current situation
Yemen is facing a re-emergence and rise in vaccine-preventable diseases and associated deaths among children. This is the result of economic decline and low incomes, displacement, and overcrowded living conditions in camps, coupled with an overwhelmed health system and low immunization rates.
Millions of children remain unreachable through routine immunization activities. According to the WHO-UNICEF National Immunization Coverage Estimate for 2022, about one third (27%) of children aged under 1 year in Yemen are not immunized against measles and rubella. Nor have these children received the minimum set of vaccines to sustain their lives.
Yemen joined the Global Polio Eradication Initiative (GPEI) in the 1990s and successfully eliminated the indigenous wild poliovirus in 2006. Yemen successfully interrupted the spread of circulating poliovirus type 2 (cVDPV2) in 2011–2012 and remained free of any polio outbreak until 2020.
The re-emergence in Yemen of poliovirus type 1 (cVDPV1), in 2020, was soon followed by the re-emergence of cVDPV2, in 2021. This has put Yemen back on the world map of 35 countries currently afflicted by this debilitating and incurable disease.

View Chart 1 in an interactive format

View Chart 2 in an interactive format
WHO vaccination efforts in Yemen
WHO works closely with Yemen’s Ministry of Public Health and Population and health partners to increase support for routine vaccination interventions. WHO also continues to work within the National Health Framework to provide technical and financial support to improve immunization rates among children.
These efforts include work to:
enhance national disease surveillance and data management, ensuring timely detection of cases;
maintain public health teams dedicated to vaccine-preventable diseases;
improve the quality and coverage rates of preventive and outbreak response campaigns;
support the implementation of the equity accelerator proposal to reduce the number of zero-dose children; and
implement integrated vaccination and outreach campaigns.
Since the re-emergence of cVDPV1 and cVDPV2, WHO has closely supported the Ministry of Public Health and Population to develop a polio outbreak response plan; implement outbreak response immunization activities; and intensify surveillance, advocacy and capacity-building efforts.
WHO support for Yemen’s national Expanded Programme on Immunization (EPI) has contributed significantly to decreasing childhood morbidity and mortality resulting from vaccine-preventable diseases. For full immunization against these deadly childhood diseases, a child needs only 5 visits to the health facility in the first year of life, plus a single visit in each of the second and fifth years of life.
About Yemen’s national EPI
Yemen’s national EPI was launched in 1974. It aims to reduce the incidence rates of maternal and neonatal tetanus, ensure full immunization of children aged under 1 year, and extend all new vaccines and preventive health measures to children in all of Yemen’s districts, to reduce the number of deaths associated with vaccine-preventable diseases.
Various new vaccines for childhood diseases have since been introduced. Currently, EPI offers every child in Yemen immunization against diphtheria, pertussis, tetanus, poliomyelitis, measles, rubella, pneumococcal disease , hepatitis B, diarrhoea caused by rotavirus , Hib pneumonia and tuberculosis. A surveillance system has also been set up within Yemen’s EPI, to report, investigate and respond to any outbreak related to vaccine-preventable diseases.
EPI has a set of standard indicators to evaluate progress on a quarterly, biannual and annual basis. This includes indicators for Pentavalent vaccine 1 and 3 coverage, to evaluate the accessibility of the services; and dropout rate. This helps assess the use of services by the community and the effectiveness of the surveillance system.